Antimicrobial resistance

By Jennifer Davis and Celia Marr

Using antimicrobials as effectively as possible helps to reduce their use overall. For septic arthritis, intravenous regional perfusion of antimicrobials can achieve very high concentrations within a specific limb. This involves placing a temporary tourniquet to reduce blood flow away from the area while the antimicrobial is injected into a nearby blood vessels. The technique is suitable for some but not all antimicrobial drugs.
Growing numbers of bacterial and viral infections are resistant to antimicrobial drugs, but no new classes of antibiotics have come on the market for more than 25 years. Antimicrobial-resistant bacteria cause at least 700,000 human deaths per year according to the World Health Organization (WHO). Equivalent figures for horses are not available, but where once equine vets would have very rarely encountered antimicrobial-resistant bacteria, in recent years this serious problem is a weekly, if not daily, challenge.
The WHO has for several years now, designated a World Antibiotic Awareness Week each November and joining this effort, British Equine Veterinary Association and its Equine Veterinary Journal put together a group of articles exploring this problem in horses.
How do bacterial populations develop resistance?
Certain types of bacteria are naturally resistant to specific antimicrobials and susceptible to others. Bacteria can develop resistance to antimicrobials in three ways: bacteria, viruses and other microbes, which can develop resistance through genetic mutations or by one species acquiring resistance from another. Widespread antibiotic use has made more bacteria resistant through evolutionary pressure—the “survival of the fittest” principle means that every time antimicrobials are used, susceptible microbes may be killed; but there is a chance that a resistant strain survives the exposure and continues to live and expand. The more antimicrobials are used, the more pressure there is for resistance to develop.
The veterinary field remains a relatively minor contributor to the development of antimicrobial resistance. However, the risk of antimicrobial-resistant determinants travelling between bacteria, animals and humans through the food chain, direct contact and environmental contamination has made the issue of judicious antimicrobial use in the veterinary field important for safeguarding human health. Putting that aside, it is also critical for equine vets, owners and trainers to recognise we need to take action now to limit the increase of antimicrobials directly relevant to horse health.
How does antimicrobial resistance impact horse health?

This mare’s problems began with colic; she underwent surgery to correct a colon torsion (twisted gut). When the gut wall is damaged, bacteria easily spread throughout the body. The mare developed an infection in her surgical incision and in her jugular veins, progressing eventually to uncontrollable infection—resistant to all available antimicrobials with infection of the heart and lungs.
The most significant threat to both human and equine populations is multidrug-resistant (MDR) pathogens, including methicillin-resistant Staphylococcus aureus (MRSA), extended-spectrum beta-lactamase (ESBL) producing Escherichia coli, MDR Klebsiella pneumoniae, Pseudomonas aeruginosa, Enterococcus faecium, and rising MDR strains of Salmonella spp. and Clostridium difficile. In an analysis of 12,695 antibiograms collected from horses in France between 2012-2016, the highest proportion (22.5%) of MDR isolates were S. aureus. Identification of ESBL E.coli strains that are resistant to all available antimicrobial classes has increased markedly in horses. In a sampling of healthy adult horses at 41 premises in France in 2015, 44% of the horses shed MDR E.coli, and 29% of premises shedding ESBL isolates were found in one third of the equestrian premises. Resistant E. coli strains are also being found in post-surgical patients with increasing frequency.

Rhodococcus equi is a major cause of illness in young foals. It leads to pneumonia and lung abscesses, which in this example have spread through the entire lung. Research from Kentucky shows that antimicrobial resistance is increasingly common in this bacterial species.
Of major concern to stud owners, antimicrobial-resistant strains of Rhodococcus equi have been identified in Kentucky in the last decade, and this bacteria can cause devastating pneumonia in foals. Foals that are affected by the resistant strains are unlikely to survive the illness. One of the leading authorities on R equi pneumonia, Dr Monica Venner has published several studies showing that foals can recover from small pulmonary abscesses just as quickly without antibiotics, and has pioneered an ‘identify and monitor’ approach rather than ‘identify and treat’. Venner encourages vets to use ultrasonography to quantify the infected areas within the lung and to use repeat scans, careful clinical monitoring and laboratory tests to monitor recovery. Antimicrobials are still used in foals, which are more severely affected, but this targeted approach helps minimise drug use.
What can we do to reduce the risk of antimicrobial resistance?

Faced with a coughing horse, trainers will often pressure their vet to administer antibiotics, hoping this will clear the problem up quickly. Many respiratory cases will recover without antibiotics, given rest and good ventilation.
The simple answer is stop using antimicrobials in most circumstances except where this is absolutely avoidable. In training yards, antimicrobials are being over-used for coughing horses. Many cases are due to viral infection, for which antibiotics will have little effect. There is also a tendency for trainers to reach for antibiotics rather than focusing on improving air quality and reducing exposure to dust. Many coughing horses will recover without antibiotics, given time. Although it has not yet been evaluated scientifically, adopting the ‘identify and monitor’ approach, which is very successful in younger foals, might well translate to horses in training in order to reduce overuse of antimicrobials.
Vets are also encouraged to choose antibiotics more carefully, using laboratory results to select the drug which will target specific bacteria most effectively. The World Health Organization has identified five classes of antimicrobials as being critically important, and therefore reserved, antimicrobials in human medicine. The critically important antimicrobials which are used in horses are the cephalosporins (e.g., ceftiofur) and quinolones (e.g., enrofloxacin), and the macrolides, which are mainly used in foals for Rhodococcal pneumonia. WHO and other policymakers and opinion leaders have been urging vets and animal owners to reduce their use of critically important antimicrobials for well over a decade now. Critically important antimicrobials should only be used where there is no alternative, where the disease being treated has serious consequences and where there is laboratory evidence to back up the selection. British Equine Veterinary Association has produced helpful guidelines and a toolkit, PROTECT-ME, to help equine vets achieve this.
How well are we addressing this problem?….


BUY THIS ISSUE IN PRINT OR DOWNLOAD
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
Bleeders - the facts, fiction and future direction
By Dr. David Marlin

We are now approaching half a century since Bob Cook pioneered the use of the flexible fibreoptic endoscope, which allowed examination of the respiratory tract in the conscious horse. One of the important outcomes of this technique was that it opened the door to the study of ‘bleeding’ or exercise-induced pulmonary haemorrhage (EIPH). But nearly 50 years on the irony is perhaps that whilst we have become good at describing the prevalence of EIPH and some of the factors that appear to increase the severity of EIPH within individual horses, we still lack a clear understanding of the condition and how to manage it. I use the term manage rather than treat or prevent as our knowledge of EIPH must show us that EIPH cannot be stopped entirely; it is a consequence of intense exercise. The other irony is that in the past 50 years, by far the majority of research into the management of EIPH has focussed on the use of the diuretic furosemide. Whilst we have good evidence from controlled studies that furosemide reduces the severity of EIPH on a single occasion, we still lack good evidence to suggest that furosemide is effective when used repeatedly during training and or racing; and there is also evidence to the contrary.
Let’s review some basic facts about EIPH, which should not be contentious.
EIPH is the appearance of blood in the airways associated with exercise.
EIPH occurs as a result of moderate to intense exercise. In fact, EIPH has been found after trotting when deep lung wash (bronchoalveolar lavage or BAL) is done after exercise.
EIPH most often involves the smallest blood vessels (capillaries) but can sometimes and less commonly be due to the rupture of larger blood vessels.
The smallest blood vessels are extremely thin. Around 1/100th the thickness of a human hair. But this extremely thin membrane is also what allows racehorses such as thoroughbreds, standardbreds and Arabs to use oxygen at such a high rate and is a major reason for their athleticism.
EIPH is a progressive condition. The chance of seeing blood in the trachea after exercise increases with time in racing.
EIPH is variable over time, even when horses are scoped after the same type of work.
If you ‘scope a horse after three gallops in a row, you can expect to see blood in the trachea on at least one occasion.
EIPH damage to the lungs starts at the back and top, and over time moves forward and down and is approximately symmetrical.
Following EIPH the lung becomes fibrotic (as scar tissue), stiffer and does not work as well. The iron from the blood is combined with protein and stored permanently in the lung tissue where it can cause inflammation.
High blood pressure within the lung is a contributing factor in EIPH. Horses with higher blood pressure appear to suffer worse EIPH.
There is also evidence that upper airway resistance and breathing pattern can play a role in EIPH.
Airway inflammation and poor air quality may increase the severity of EIPH within individual horses.
Increasing severity of EIPH appears to have an increasing negative effect on performance.
Visible bleeding (epistaxis) has a very clear and marked negative effect on performance.
In order to make progress in the management of EIPH (i.e., to minimise the severity of EIPH in each individual), there are certain steps that trainers can take based on the information we have to date.
These include:

Ensuring good air quality in stables
Regular respiratory examination and treatment of airway inflammation
Reduced intensity of training during periods of treatment for moderate to severe airway inflammation
Extended periods of rest and light work with a slower return to work for horses following viral infection
Addressing anything that increases upper airway resistance (e.g., roaring, gurgling)
Avoiding intense work in cold weather
Avoiding extremes of going
Limiting number of training days in race preparation and increasing interval between races

Endoscopy
FUTURE OPPORTUNITIES IN UNDERSTANDING AND MANAGING EIPH
We have to accept EIPH as a normal consequence of intense exercise in horses. Our aim should be to reduce the severity to a minimum in each individual horse. However, there are areas in which we still need a much greater scientific understanding.
What actually causes the capillaries to leak or rupture?…
TO READ MORE —
BUY THIS ISSUE IN PRINT OR DOWNLOAD
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
An Introduction to the Functional Aspects of Conformation

By Judy Wardrope
Why is one horse a sprinter and another a stayer? Why is one sibling a star and another a disappointment? Why does one horse stay sound and another does not? Over the course of the next few issues, we will delve into the mechanics of the racehorse to discern the answer to these questions and others. We will be learning by example, and we will be using objective terminology as well as repeatable measures. This knowledge can be applied to the selection of racing prospects, to the consideration of distance or surface preferences and, of course, to mating choices.
Introducing a different way of looking at things requires some forethought. Questions need to be addressed in order to provide educational value for the audience. How does one organise the information, and how does one back up the information? In the case of equine functionality in racing, which horses will provide the best corroborative visuals?



After considerable thought, these three horses were selected: Tiznow (Horse #1) twice won the Breeders’ Cup Classic (1¼ miles) ; Lady Eli (Horse #2) won the Juvenile Fillies Turf and was twice second in the Filly and Mare Turf (13/8 miles); while our third example (Horse #3) did not earn enough to pay his way on the track. Let’s see if we can explain the commonalities and the differences so that we can apply that knowledge in the future.
Factors for Athleticism
If we consider the horse’s hindquarters to be the motor, then we should consider the connection between hindquarters and body to be the horse’s transmission. Like in a vehicle, if the motor is strong, but the transmission is weak, the horse will either have to protect the transmission or damage it.
According to Dr. Hilary M. Clayton (BVMS, PhD, MRCVS), the hind limb rotates around the hip joint in the walk and trot and around the lumbosacral joint in the canter and gallop. “The lumbosacral joint is the only part of the vertebral column between the base of the neck and the tail that allows a significant amount of flexion [rounding] and extension [hollowing] of the back. At all the other vertebral joints, the amount of motion is much smaller. Moving the point of rotation from the hip joint to the lumbosacral joint increases the effective length of the hind limbs and, therefore, increases stride length.” From a functional perspective, that explains why a canter or gallop is loftier in the forehand than the walk or the trot.
In order to establish an objective measure, I use the lumbosacral (LS) gap, which is located just in front of the high point of the croup. This is where the articulation of the spine changes just in front of the sacrum, and it is where the majority of the up and down motion along the spine occurs. The closer a line drawn from the top point of one hip to the top point of the other hip comes to bisecting this palpable gap, the stronger the horse’s transmission. In other words, the stronger the horse’s coupling.

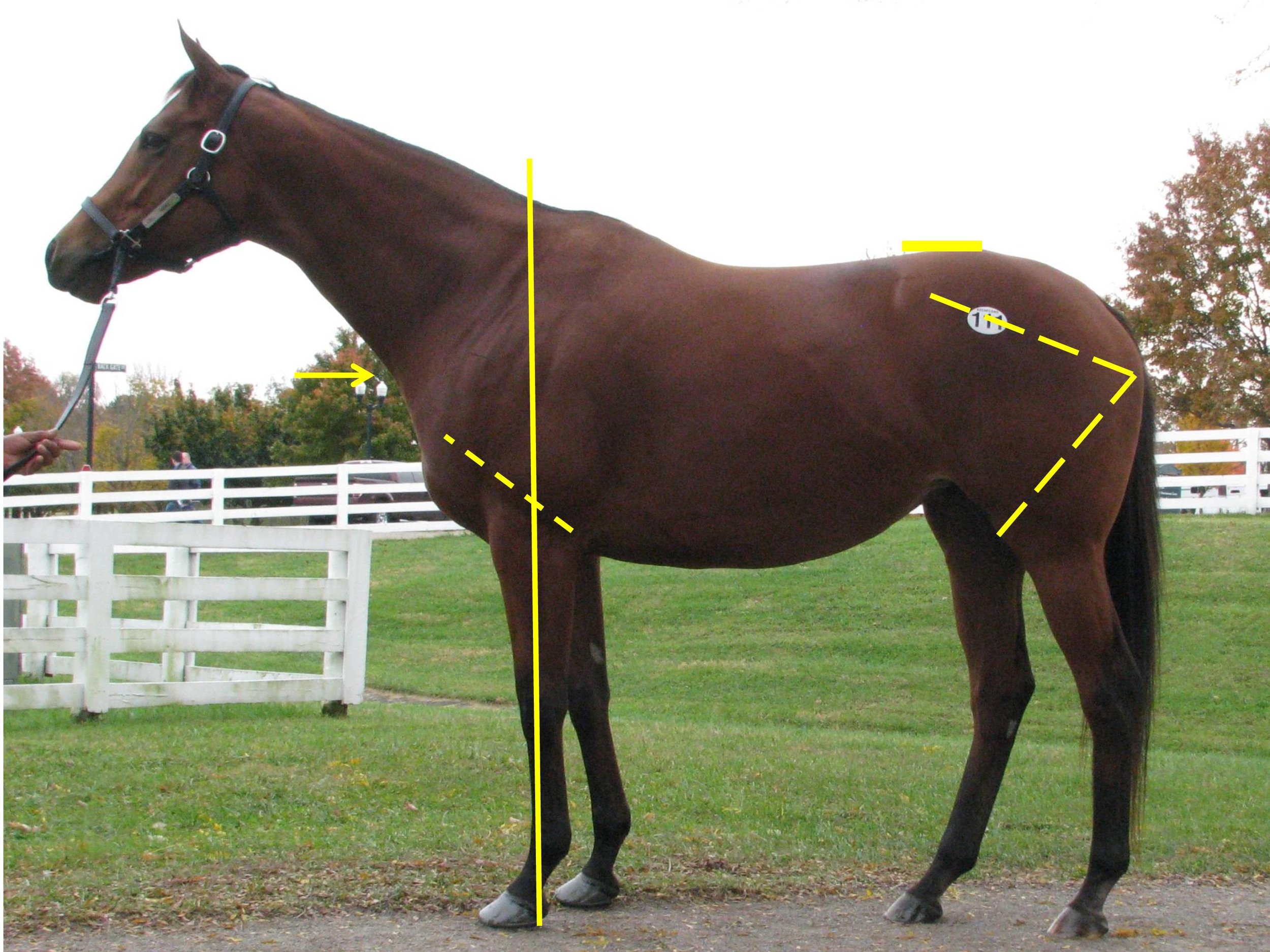
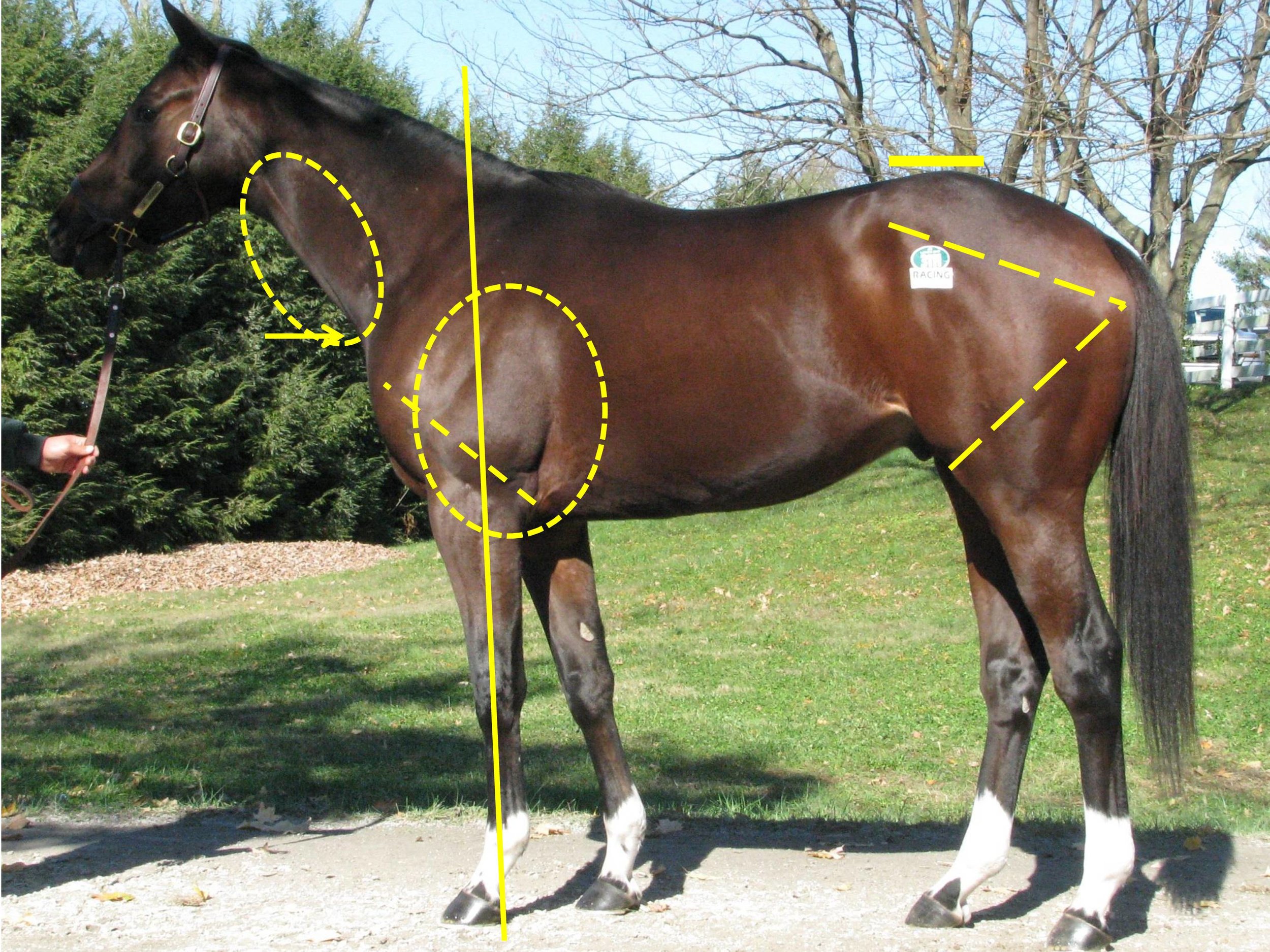
We can see that the first two horses have an LS gap (just in front of the high point of the croup as indicated) that is essentially in line with a line drawn from the top of one hip to the top of the opposing hip. This gives them the ability to transfer their power both upward (lifting of the forehand) and forward (allowing for full extension of the forehand and the hindquarters). Horse #3 shows an LS gap considerably rearward of the top of his hip, making him less able to transfer his power and setting him up for a sore back.
You may also notice that all three of these sample horses display an ilium side (point of hip to point of buttock), which is the same length as the femur side (point of buttock to stifle protrusion)—meaning that they produce similar types of power from the rear spring as it coils and releases when in stride. We can examine the variances in these measures in more detail in future articles, when we start to delve into various ranges of motion as well as other factors for soundness or injury.
Factors for Distance Preferences…
TO READ MORE —
BUY THIS ISSUE IN PRINT OR DOWNLOAD
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
Equine Pain: how can we recognise it and which painkiller should we use?

By Professor Celia Marr
We can all agree that alleviating pain in our patients is an important goal, but we may not be as good as we might hope at recognising pain in horses. Studies have shown that there is considerable variation in the scores vets assign when asked to predict how much pain they expect to see with specific clinical conditions.
Acute severe pain is perhaps most easily recognised by horsemen and vets; signs of severe colic, such as rolling, are usually very obvious. Low-grade pain, and pain not associated with abdominal disease can be more difficult to detect and go unrecognised. In particular, intra-thoracic pain and pain associated with injuries to the thoracic cage, withers and spine can be difficult to pinpoint.

This horse is clearly showing signs of abdominal pain—colic. It is lying down, has been rolling and is looking at its flank.
Comfortable horses interact with their environment, look out over their stable door and eat willingly. Reluctance to move and restlessness indicate pain while looking at the flank, and kicking at the abdomen all suggest localised pain. Behaviours such as lifting hindlimbs, extending head, lateral and/or vertical head movements and pawing are also observed in uncomfortable horses.
Facial expression and pain
In humans, facial expressions are an important part of nonverbal communication. The Horse Grimace Scale has been developed to help identify subtle pain in horses. The grimace scale is easy to learn, can be applied quickly and takes into account our natural human tendency to focus on the face when evaluating both human and non-humans around us. This scale looks at ear position, tension around the eyes, tension in the chewing muscles and shape of the nostrils which tend to be held in a strained position if in pain. More complex pain scales incorporate facial expression with head position, flehmen, yawning, teeth grinding and interaction with people.


These scales were used in a recent Equine Veterinary Journal article looking at optimal methods to provide anaesthesia for castration. But, the focus on a strained facial expression, ears held back and lack of interaction with people can easily be misinterpreted as poor temperament. It is well worth trainers taking time to make sure their staff are educated on how to recognise signs of pain, as these sorts of clinical signs might indicate important conditions such as gastric ulcers, pneumonia or even musculoskeletal conditions such as fractured ribs. Yard staff should be encouraged to give horses the benefit of the doubt and report any apparent poor temperament so that veterinary investigations can be undertaken to get to the bottom of the problem. Similarly, these signs can be used to monitor horses after potentially painful procedures such as following surgery or castration.
What do we know about analgesic use in equine practice?
There is an increasingly large number of painkillers, also known as analgesics, which are either licensed for use in the horse or supported by research evidence. But it is likely that most equine vets use a relatively small range. British Equine Veterinary Association (BEVA) has recently tasked a team of its members to look at the evidence with underpin best practice for selections of analgesics in common clinical scenarios. This group is chaired by Professor Mark Bowen of the University of Nottingham and has been working for two years now and has collected evidence from the veterinary literature; and in parallel the group has consulted BEVA members to develop robust recommendations. The BEVA Clinical Practice Guidelines report on analgesia will be published soon and looks at the most effective analgesia in horses undergoing routine castration, horses with acute colic, orthopaedic pain and in horses with chronic pain that does not respond to standard non-steroidal anti-inflammatory drugs (NSAIDs) such as phenylbutazone (aka “Bute”). In making their recommendations around use of analgesics in horses, the BEVA team considered both the effectiveness of each analgesic drug, its safety and potential for side-effects.
What are the desirable characteristics of analgesic drugs?
The ideal analgesic has predictable effect and duration, minimal side effects and is easy to prescribe, purchase and administer, lacking any impact on the horse’s future status for human consumption. Of course, the ideal analgesic does not exist. To a large extent, the most appropriate analgesic will be dictated by the specific clinical indication.
Analgesia in colic
With colic, predictable level of analgesia and duration of action are key characteristics. The BEVA team found moderate evidence that flunixin provides superior analgesia to meloxicam and phenylbutazone in horses with colic. However, effective analgesia is desirable but very potent drugs are usually avoided for fear of masking declining clinical status in a horse which would be best served by surgical exploration rather than controlled with extremely potent analgesics. Potential damage to the gastrointestinal tract and effects on gastrointestinal motility are critical and the impact of concurrent shock and volume depletion must be considered. Similar considerations come into play with peri-operative pain but here, the level of analgesia required may be modified by the exact surgical indication and specific procedure and with some procedures, it will be appropriate to provide very potent analgesia, for example with surgical repair of fractures or other painful orthopaedic surgeries. In these cases, multimodal analgesia may well be indicated.
Analgesia following castration
The BEVA team found robust evidence to support a recommendation that pre-operative NSAIDs should be administered prior to surgery. They also recommended that analgesia should be given for at least three days after surgery and that local anaesthetic should be infused into the testicle even when a general anaesthetic is administered. Finally, they counselled that pre-operative use of butorphanol (a commonly used component of sedative protocols) alone should not be considered adequate analgesia for horses undergoing castration.
Selection of NSAIDs for musculoskeletal pain
There is moderate evidence to indicate that phenylbutazone provides superior analgesia for hoof pain / laminitis, compared to firocoxib and meloxicam but strong evidence to show that Suxibuzone can be used as a direct replacement for phenylbutazone in chronic orthopaedic pain. The evidence supporting the use of other NSAIDs is less definitive. Meloxicam and firocoxib may be equivalent to phenylbutazone for pain associated with inflammation of the joint lining and, although studies are not conclusive, the group came to the conclusion that ketoprofen is not as effective for addressing musculoskeletal pain.
One of the key safety recommendations relating to the use of phenylbutazone was that it is the NSAID that is most likely to induce gastrointestinal adverse events (right dorsal colitis or gastric glandular ulceration). However, although other NSAIDs have less adverse intestinal effects but can all be considered as potentially ulcerogenic. Horses on long-term analgesic therapy should be monitored carefully and further investigations undertaken if they show weight loss, poor appetite or develop the more general signs of pain described above, as this might indicate that the NSAID is having adverse effects on the intestine.
The BEVA team also concluded that giving NSAIDs at doses above those generally recommended in veterinary texts and stacking (i.e., combining maximal doses of different NSAIDs) should be avoided. These practices simply increase risk with no analgesic benefit.
Alternative analgesics
Unfortunately, there are not many practical alternatives to NSAIDs. There is research ongoing looking at topical NSAIDs and alternative drugs such as paracetamol, tramadol and fentanyl. These drugs are unlikely to be in common use in horses in training but do have a place in management of horses with more severe clinical problems.
Similarly, morphine and methadone are used commonly in equine hospitals, but these Schedule 2 controlled drugs are generally not used widely in practice. Buprenorphine has been extensively researched recently and evidence is accumulating supporting its use particularly in the peri-operative patient.
Final warnings
The BEVA group’s report contained a clear warning that highly potent analgesia should only be utilised under the direct control of a veterinary surgeon who has fully evaluated a horse and having developed a therapeutic, analgesic plan that includes ongoing monitoring. It is also important to bear in mind that the best way to alleviate pain associated with a specific clinical condition is to cure the underlying cause. Painkillers should always be used with respect and not be seen as a way to patch up a horse that has an undiagnosed musculoskeletal problem or internal condition.
BUY THIS ISSUE IN PRINT OR DOWNLOAD
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
Advances in Imaging of the Equine Athletic Heart

By Francesca Worsman BVM&S MRCVS
Horserace Betting and Levy Board Senior Clinical Training Scholar in Equine Internal Medicine, Royal (Dick) School of Veterinary Studies, University of Edinburgh
Horses, through selective breeding for athletic excellence, have well-developed hearts that rarely cause problems compared to those encountered by humans. On occasions however, things go wrong. Due to their well-developed physiology, horses are at risk of a fibrillating heart (atrial fibrillation), while circumstantial evidence suggests that more severe heart rhythm abnormalities, somewhat akin to those experienced by human athletes, may cause sudden death. Ultrasound examination of the heart, known as echocardiography is a readily available tool for examining the heart and significant advances in ultrasound technology are likely to provide exciting information about the detailed function of the equine heart. A huge benefit of ultrasound is that it is non-invasive and can be carried out on a standing unsedated horse, so normal heart function is maintained during the examination.
The equine heart, like all mammalian hearts, has four chambers. The right atrium, which receives oxygen-depleted blood from the organs, passes it into the right ventricle which then pumps it to the lungs. Blood picks up oxygen in the lungs and then returns it to the left atrium, which then passes it onto the left ventricle for pumping to the organs of the body, including the muscles. Oxygen is thus delivered to the tissues and then the cycle repeats, more than 50,000 times per day! The left and right atria work in unison during heart filling (diastole), and the left and right ventricles work in unison during evacuation of blood from the heart (systole). Murmurs, often detected by veterinary surgeons when listening to hearts, are either caused by normal forward blood flow through the heart or by backflow leakage across the valves within the heart (regurgitation). Many of these murmurs are not a cause for concern, although some regurgitant murmurs are more severe and can cause problems with heart function. Similarly most heart rhythm abnormalities are innocuous and do not affect performance while others are more serious. In some horses, due to suspicion by a veterinary surgeon of a more significant problem, extensive evaluation of the heart is required; echocardiography is one of the key tools for diagnostic evaluation of the heart to assess the impact of any problems on athletic performance.

Image taken from the right side of the horse. Biplane views are on the left (4 chamber standard long axis view at top, short axis view at the bottom of the picture) and 3DE image on the right of the picture. In real-time the image can be manipulated as the heart is beating to visualise the cardiac structures from different angles. RV = right ventricle, TV = tricuspid valve, RA = right atrium, LV = left ventricle, MV = mitral valve, LA = left atrium.
Real-time three-dimensional echocardiography (3DE) is an exciting new tool that has recently become available in equine medicine and may shed light on important heart problems in horses, including those that cause poor performance. Compared to standard two dimensional echocardiography (2DE), which evaluates a single scan plane, 3DE involves the simultaneous collection of multiple scan planes from the heart to create a pyramid of scan data. 3DE is preferable to 2DE because in theory it does not rely on geometric assumptions on chamber shape to calculate chamber volumes. Also assessment of heart architecture and function (including that of valves) is likely to be more accurate as the technique provides unlimited viewing planes. Finally, for assessment of regurgitant flow, this technique should also be better because the image can be manipulated to better assess the leaky flow from those valves. In humans, for certain heart volume and muscle mass measurements, 3DE is more comparable than 2DE to cardiac magnetic resonance imaging (MRI), which is the acknowledged gold standard. Unfortunately, owing to the significantly larger size of horses, there is currently no equipment available for equine cardiac MRI. Therefore, 3DE could provide the next best option for more detailed equine cardiac evaluation.
Mitral valve regurgitation for example is commonly encountered in the equine athlete and, while often of no consequence, in more severe cases, it may lead to poor performance. Pathological consequences are due to backflow leakage causing secondary left atrial volume overload, and this will lead to an increased likelihood of atrial fibrillation. Potential advantages of 3DE in this context are more accurate assessment of the degree of volume overload, the regurgitant orifice (i.e., size of the hole!), and the valve structure and motion. Mitral valve regurgitation can be easily confirmed by 2DE, however it can be more difficult to ascertain the cause and severity. With 3DE, the software allows manipulation and therefore anatomic evaluation of the valves from many angles including ‘face-on‘ views. This results in more detailed evaluation of subtle abnormal valve motion and confirmation of suspected findings, which can’t be reliably detected by 2DE - eg. mitral valve thickening, mitral valve prolapse or ruptured chordae tendineae as the cause of mitral valve disease. Geometric assumptions on volume are avoided as much more structural data is obtained.
A few specialist centres worldwide currently offer 3DE imaging for horses including the Equine Hospital at the Royal (Dick) School of Veterinary Studies, University of Edinburgh. In equine medicine we are still at an early stage of using 3DE as it is not validated in horses, therefore it is mostly used in research at the moment as opposed to routine diagnosis. As part of my research at Edinburgh, sponsored by the Horserace Betting and Levy Board, I have been assessing the left atrial volume using 3DE from thoroughbreds in training. One of my aims was to determine the variability of equine left atrial volume measurement using a special 3DE software analysis package to see how much variation there was between successive 3DE measurements by the same person. Forty-four National Hunt thoroughbreds in training were scanned to obtain the 3DE views of this chamber. We then graded them to exclude images of reduced image quality so that we were only assessing good quality images of the left atrium. In total 24 horses were included—aged 4-9 yrs, weighing 411-534kg. I analysed the images retrospectively, after the horses were scanned. I didn’t include any horses with grade >3/6 heart murmurs. This was because we first need to validate 3DE with normal, healthy hearts. Random generated order measurements were obtained by a single person on four occasions. Real-time three-dimensional end-systolic (ESV) and end-diastolic (EDV) left atrial volumes were measured using 3DE software, and the results were then statistically analysed.
TO READ MORE —
BUY THIS ISSUE IN PRINT OR DOWNLOAD
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
Skin-deep: overcoming barriers for effective transdermal drug delivery

By Roger Smith
Ancient art, modern science
One shared medicinal practice amongst disparate ancient societies was the application of primitive ointments to the skin to treat almost all and any ailments. A vast plethora of poultices and plasters have been described, including in Babylonian and Greek medicine texts1 amongst others, suggesting that the magical health-restoring powers of ointments were well-recognised to traverse the skin. Thus, it was no coincidence that the skin was the preferred therapeutic route over surgical (and oral) intervention since the former method was likely to result in reduced mortality rates compared to the latter; undoubtedly an important consideration, given that the top ancient physicians were likely charged with the health of the royal courts.
Although the art of transdermal delivery of medicines dates back millennia, it is only in more recent times that the science of transdermal drug delivery in man has advanced significantly2. The choice of modern drugs for topical applications is, however, relatively limited compared to the seemingly infinite choice available for oral delivery. This is perhaps not surprising since the gut is an organ that has evolved with the main purpose of absorbing food (chemicals when it comes to it) whereas the skin, despite being the largest organ, has evolved primarily as a protective layer to prevent desiccation of underlying tissues and to keep out harmful environmental chemicals. As this includes medicinal drugs, the pursuit of transdermal administration would appear, at first sight, to be an illogical choice. However, there are several compelling reasons why transdermal delivery routes are an important alternative to pills, injections or inhalation routes:
It avoids poor absorption after oral ingestion—especially in animals, the absorption of a drug can vary between the omnivore (e.g., human) and herbivore (e.g., horse) stomach.
It avoids first-pass effect where the blood circulation from the gut passes through the liver to remove absorbed drugs.
It can reduce systemic drug levels to minimise adverse effects.
The design of sustained release formulations overcomes the frequent dosing necessitated by oral and injectables to achieve constant drug levels.
It enables ease and efficacy of drug withdrawal.
Transdermal drug delivery is painless and non-invasive, thereby potentially allowing longer treatment when daily injection is unacceptable or impractical.
It has the potential to target local administration such as for the treatment of flexor tendon disease because the tendons are subcutaneous.
Challenges for transdermal drug applications
The skin is made up of three key layers: the epidermis, dermis and hypodermis (figure 1) and the water-attracting (hydrophilic) or water-repelling (hydrophobic) properties within each raise unique challenges for topical or transdermal drug applications.

Figure 1 – Anatomy of the skin with expanded illustration showing the cells of the stratum corneum (‘bricks’) embedded in lipid matrix (‘mortar’).
Topical applications, such as insect repellents and sunscreen creams, target the surface of the skin or deliver a drug locally such as for the control of inflammation (insect bite or reaction to an allergen). In contrast the aim of transdermal, or subcutaneous, applications are to deliver the drug deeper to either an adjacent organ, or, more commonly, to the blood circulation as an alternative to oral or needle routes to reach distant organs. The main barrier to local or transdermal delivery is the outermost layer of the skin, called the stratum corneum in the epidermis (figure 1). This consists of dead skin cells, the corneocytes, that combine with lipid bilayers into a tightly packed “bricks-and-mortar” layer that form alternating hydrophilic (the water rich corneocytes) and hydrophobic (lipid bilayer) regions (figure 1). The stratum corneum therefore not only forms a mechanically robust layer but also presents a challenge in designing drugs with chemical properties that can negotiate their way into and through these contrasting hydrophobic and hydrophilic environments to reach the lower region of the epidermis. The epidermis consists of living skin cells but has no blood vessels for the drug to diffuse into, so instead the drug must penetrate further to the dermis where it can finally enter the bloodstream or the subcutaneous layers.
Routes for drugs through the skin

Most transdermal drugs are designed so that they diffuse through the skin in a passive fashion. The routes for drug can be through the skin cells (transcellular), around them (intercellular) or using the skin components hair follicles, sweat glands and sebaceous glands (produce lipids) to bypass the stratum corneum (so-called ‘appendageal’ routes).
Transcellular route: Drugs pass through the corneocytes of the stratum corneum rather than the lipid ‘mortar’ that surrounds them (figure 2). However, the drug has to exit the cell to enter the next corneocyte and therefore through the skin. It means that it has to encounter the external hydrophobic environment between the cells multiple times as it moves through the alternating cell and lipid layers of the epidermis. Drugs therefore have to have balanced hydrophilic and hydrophobic properties to enable this to happen.

Figure 2 – Path of molecules through (A) the stratum corneum for the transcellular route (Note: the drug has to enter and exit the aqueous environment of the cells into the surrounding lipid matrix requiring an ability to be soluble in both); (B) Intercellular route (Note: the tortuous path for molecules passing through the stratum corneum via this route which delays diffusion.
Intercellular route: The drug predominantly diffuses through the lipid rich ‘mortar’ around the corneocytes of the epidermis. This lipid matrix can form a continuous route through the epidermis (avoiding entering the cells), but this route has been suggested to be less efficient because it increases the distance 50-fold3 compared to the direct route through the stratum corneum due to the interdigitating brick and mortar arrangement (figure 2). Again, the chemical formulation used to carry the drug is important and drugs that more readily dissolve in lipids benefit from this route.
Appendageal route: The hair, sweat glands and sebaceous glands provide a direct channel to the deep layers of the skin circumventing the hazardous barriers of the epidermis and dermis. The main challenge for this relatively easy route is that the amount of drug that can be taken up is limited by the density of hair follicles and sweat glands, although in haired animals, such as the horse, the density can be as high as 1-5% of the skin surface area. Furthermore, sweat from an active sweat gland would be travelling against the direction of drug flow, washing out the drug and its carrier and severely limit drug uptake. It is likely that all skin applications use this appendageal route as it’s unavoidable but probably more efficient for drugs that are large molecules.
TO READ MORE —
BUY THIS ISSUE IN PRINT OR DOWNLOAD
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!

Ulcer medication: are the products to treat that different?


By Celia Marr
Stomach ulcers are not all the same
Racehorse trainers and their vets first began to be aware of stomach ulcers over 20 years ago. The reasons why we became aware of ulcers are related to technological advances, which produced endoscopes long enough to get into the equine stomach. At that time, scopes were typically about 2.5m long and were most effective in examining the upper area of the stomach, which is called the squamous portion. Once this technology became available, it was quickly appreciated that it is very common for racehorses to have ulcers in the squamous portion of the stomach.

Fig 1. The equine stomach has two regions: the upper region is the squamous portion and the lower region is the glandular portion. The squamous portion is lined by pale pink tissue which is susceptible to acid damage. The glandular portion is lined by darker purple tissue. Acid is produced in this region. In this horse, the stomach lining is healthy and unblemished. The froth is due to saliva which is continuously swallowed.
The equine stomach has two main areas: the squamous portion and the glandular portion. The stomach sits more or less in the middle of the horse, immediately behind the diaphragm and in front of and above the large colon. Imagine the stomach as a large balloon with the oesophagus—the gullet—entering halfway up the front side and slightly to the left of the balloon-shaped stomach and the exit point also coming out the front side but slightly lower and to the right side. The tissue around the exit—the pylorus—and the lower one-third, the glandular portion, has a completely different lining to the top two-thirds, the squamous portion.
The stomach produces acid to start the digestive process. Ulceration of the squamous portion is caused by this acid. Like the human oesophagus, the lining of the squamous portion has very limited defences against acid. But, the acid is actually produced in the lower, glandular portion. The position of the stomach is between the diaphragm, which moves backwards as the horse breathes in and the heavy large intestine which tends to push forwards as the horse moves. During exercise, liquid acid produced at the bottom of the stomach is squeezed upwards onto the vulnerable squamous lining. It makes sense then that the medications used to treat squamous ulcers are aimed at blocking acid production.
Lesions in the glandular portion of the stomach are less common than squamous ulcers. The acid-producing glandular portion has natural defences against acid damage including a layer of mucus and local production of buffering compounds. At this point, we actually know relatively little about the causes of glandular disease, but it is becoming increasingly obvious that disease in the glandular portion is very different from squamous disease. Often, it is more difficult to treat.

Fig 2. This horse shows signs of discomfort. She carries her head low, her ears are back a little, and the muscles of the face are clenched, affecting the shape of the nostrils and eye.
Stomach ulcers can cause a wide range of clinical signs. Some horses seem relatively unaffected by fairly severe ulcers, but other horses will often been off their feed, lose weight, and have poor coat quality. Some will show signs of abdominal discomfort, particularly shortly after eating. Other horses may be irritable—they can grind their teeth or they may resent being girthed. Additional signs of pain include an anxious facial expression, with ears back and clenching of the jaw and facial muscles and a tendency to stand with their head carried a little low.
Assessing ulcers
Ulcers can only be diagnosed with endoscopy. A grading system has been established for squamous ulcers, which is useful in making an initial assessment and in documenting response to treatment.
Grade 0 = normal intact squamous lining
Grade 1 = mild patches of reddening
Grade 2 = small single or multiple ulcers
Grade 3 = large single or multiple ulcers
Grade 4 = extensive, often merging with areas of deep ulceration




Fig 3. Grade 1 squamous ulcers which are mild patches of reddening.
Fig 4. Grade 2 squamous ulcers—there are several of these, but they are all small.
Fig 5. Grade 3 squamous ulcers—these are larger, and there are several.
Fig 6. Grade 4 squamous ulcers—there are extensive deep ulcers with active haemorrhage.
Although it is used for research purposes, this grading system does not translate very well to glandular ulcers where typically, lesions are described in terms of their severity (mild, moderate or severe), distribution (focal, multifocal or diffuse), thickness (flat, depressed, raised or nodular) and appearance (reddening, haemorrhagic or fibrinosuppurative). Fibrinosuppurative suggests that inflammatory cells or pus has formed in the area. Focal reddening can be quite common in the absence of any clinical signs. Nodular and fibrinosuppurative lesions may be more difficult to treat than flat or reddened lesions. Where the significance of lesions is questionable, it can be helpful to treat the ulcers and repeat the endoscopic examination to determine whether the clinical signs resolve along with the ulcers.


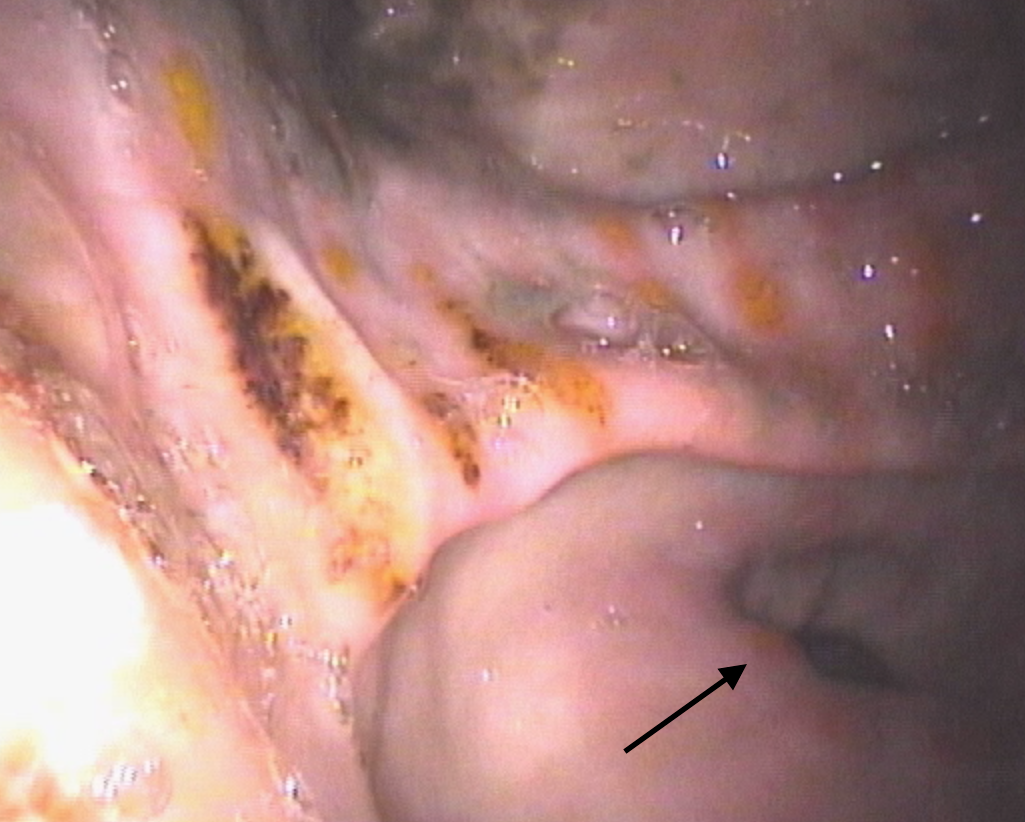

Fig 7. The glandular tissue around the pylorus (or exit point) has reddened patches. This is of questionable clinical relevance, and many horses will show no signs associated with these lesions.
Fig 8. There are dark red patches of haemorrhage in the glandular tissue of the antrum—the region adjacent to the pylorus—which is the dark hole toward the bottom of this image.
Fig 9.This horse has moderate to severe glandular disease. There are depressed suppurative (yellow) areas several of which also have haemorrhage. Nearer to the pylorus there is reddening and raised, swollen areas (arrow).
Fig 10. This horse has moderate to severe glandular disease. The majority of lesions are depressed and haemorrhagic.
Medications for squamous ulcers
Because of the prevalence and importance of gastric ulcers, Equine Veterinary Journal publishes numerous research articles seeking to optimise treatment. The most commonly used drug for treatment of squamous ulcers is omeprazole. A key feature of products for horses is that the drug must be buffered in order to reach the small intestine, from where it is absorbed into the bloodstream in order to be effective. Until recently only one brand was available, but there are now several preparations on the market and researchers have been seeking to show whether new medicines are as effective as the original brand. There is limited information comparing the new products, and this information is essential to determine whether the new, and often cheaper, products should be used.
A team of researchers formed from Charles Sturt University in Australia and Louisiana State University in the US has compared two omeprazole products given orally. A study reported by Dr Raidal and her colleagues, showed that not only were plasma concentrations of omeprazole similar with both products, but importantly, the research also showed that gastric pH was similar with both products and both products reduced summed squamous ulcer scores. Both the products tested in this trial are available in Australia and, although products on the market in UK have been shown to achieve similar plasma concentrations and it is therefore reasonable to assume that they will be beneficial, as yet, not all of them have been tested to show whether products are equally effective in reducing ulcer scores in large-scale clinical trials. Trainers should discuss this issue with their vets when deciding which specific ulcer product they plan to use in their horses.
Avoiding drugs altogether and replacing this with a natural remedy is appealing. There is a plethora of nutraceuticals around and anecdotally, horse owners believe they may be effective. One such option is aloe vera that has antioxidant, anti-inflammatory and mucus stimulatory effects which might be beneficial in a horse’s stomach. Another research group from Australia, this time based in Adelaide, has looked at the effectiveness of aloe vera in treating squamous ulcers and found that, although 56% of horses treated with aloe vera improved and 17% resolved after 28 days, this compared to 85% improvement and 75% resolution in horses given omeprazole. Therefore, Dr Bush and her colleagues from Adelaide concluded treatment with aloe vera was inferior to treatment with omeprazole.
Medications for glandular ulcers….
TO READ MORE —
BUY THIS ISSUE IN PRINT OR DOWNLOAD
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
Equine Herpesvirus-1 : An Elusive Target

By Neil Bryant
Infectious diseases are not uncommon in racehorses in training, breeding stock, and pleasure horses. Some of the more serious diseases can be financially devastating to the animal’s owners and to the equine industry on the whole. Viruses belonging to the herpesvirus family cause some of the most well characterized equine infectious diseases, and the most problematic of these is equine herpesvirus 1 (EHV-1; species Equid alphaherpesvirus 1). EHV-1 is ubiquitous in most horse populations in the world. It is responsible for major economic and welfare problems causing respiratory disease, neurological disease (mainly seen in adult horses), and abortion and neonatal foal death in pregnant mares.
This was most notably highlighted by the multiple abortion outbreak recorded in Hertfordshire, England, between February and April 2016 in fully vaccinated animals (http://www.aht.org.uk/cms-display/interim-report16-april2.html). Studies have determined that EHV-1 is a common cause of abortion. Occasional cases have also been linked to EHV-4 infection, but this is much rarer and doesn’t account for episodes of multiple abortion, as is seen occasionally with EHV-1.
The virus
EHV-1 was first isolated from an equine abortion in the U.S. in the 1930s. At the time of first isolation the vets weren’t sure what it was, but they knew it was infectious. Subsequent genetic analysis much later led to the classification of the virus in the genus Varicellovirus (family Herpesviridae), together with its close relatives equine herpesvirus 4 (EHV-4; species Equid alphaherpesvirus 4) and equine herpesvirus 8 (EHV-8; species Equid alphaherpesvirus 8). Interestingly it is grouped with, and is therefore genetically similar to, the human herpesvirus responsible for chickenpox, the Varicella Zoster virus. Initial infection of horses was thought to occur around weaning, when virus-neutralizing antibodies transferred to the foal from the mare’s colostrum had declined enough to make them susceptible to infection. However, virus has been isolated from foals as young as seven days old with high antibody levels but without any significant clinical signs. Immunity to re-infection after primary infection is relatively short-lived, lasting between three-six months, but it is rare for naturally infected mares to abort in consecutive pregnancies.
TO READ MORE --
BUY THIS ISSUE IN PRINT OR DOWNLOAD -
Why not subscribe?
Don't miss out and subscribe to receive the next four issues!
Castrating racehorses: A routine procedure not without its pitfalls

By Tom O’Keeffe
A recent study published in the Equine Veterinary Journal assessed the routine procedure of gelding and the complications associated with this procedure. The research was a retrospective study of horses castrated at the Sha Tin training complex in Hong Kong, between July 2007 and July 2012.
Hong Kong is a unique training and racing environment, and all horses training and racing there are imported, as there is no breeding in the region. Fillies are rarely imported. The majority of colts are castrated at some stage in their career, and open standing castration (OSC) is the method of choice by the vets of the Hong Kong Jockey Club (HKJC). Until now, nobody has looked at the prevalence of complications following castration of horses at the HKJC. This recently published study aimed to describe the prevalence and severity of complications in the 30 days following castration.
Reasons for gelding a racehorse in training
Most trainers perceive geldings as easier to train than colts, and if the horse has not shown enough ability for a stud career to beckon, there is little to lose by gelding. In Hong Kong, due to the unique environment the horses live in, there is an added incentive to geld these horses sooner rather than later. Once gelded, their management becomes significantly more straightforward.
Castration Method Options
Three surgical techniques are commonly used for equine castration: 1) open, in which the parietal tunic surrounding the testicle is incised and, usually, retained; 2) closed, where the portion of the parietal tunic surrounding the testis and distal spermatic cord is removed, and 3) half closed, where an incision is made through the exposed parietal tunic at the cranial end of the testis or distal end of the spermatic cord allowing the testis and part of the spermatic vasculature to be prolapsed through the incision prior to removal.
In most cases, racehorse castration is done standing via the open technique under local anesthetic, with sedation and pain relief as necessary. The testicles and spermatic cords are first injected with local anesthetic to numb the region. Once the tissues are totally desensitized, a slash incision is made into the scrotum. The testicle is exteriorized, and it is removed with a surgical instrument called an emasculator. The emasculator has a set of interlocking crushing blades with a cutting blade placed at the bottom of the array. Once the testicular cord is clamped in the emasculator the testicle will usually fall off, but the cord is retained within the interlocking crushing blades for approximately one to two minutes. This creates trauma to the tissues, which causes them to swell once the crush is released, reducing blood flow. The second effect of the emasculators is for the blood to be held in position long enough to begin the clotting process, which carries on once the clamp is removed.
An alternative method of castration is to anesthetize the horse and carry out the procedure with the horse on its back, as a completely sterile operation in an operating room. This has the advantage of minimal post-castration swelling as there is no infection in the area, which can be a common problem with standing open castrations. In horses who are cryptorchids (ridglings), which is when there is only one descended testicle in the scrotum, standard open standing castration is contraindicated. These horses require either castration under general anesthetic or testicle removal under standing surgery via laparoscopy (inserting a camera and instruments into the abdomen to remove testicle via a surgical incision).
Complications of Castration
As with all intrusive surgical procedures, there is the potential for things to go wrong. While the castration procedure is relatively straightforward, post-operative complications including excessive edema of the scrotum and surrounding tissues, infection and fever, hemorrhage, lameness, hydrocele formation, peritonitis, eventration, penile paralysis, scirrhous cord formation, and death have been recognized.
With castrations done under general anesthetic, there are all the attendant risks of putting a 1000lb animal on its back and up again. All anesthesia carries a risk of death in the horse. This has been calculated as approximately 1% in equine practice, and can be as low as 0.5% in the major well-equipped equine hospitals. In addition to this, occasional cases show prolonged bleeding after the surgery, which results in significant swelling that sometimes has to be resolved by opening the scrotal sac.

Intestine is prolapsing through the castration site - this severe castration complication requires immediate veterinary attention.
For standing castrations, some of the problems encountered include prolonged bleeding, which can occur irrespective of the length of time the cord has been clamped for. This can become serious enough to require a further surgery to identify the bleeding vessels and tie them off, but thankfully this is rare. Another rare complication is herniation of intestines through the potential space left in the inguinal canal with removal of the testicle. The intestines can either get trapped under the skin producing severe colic, or worse still, dangle out of the abdomen and become contaminated. This presents a very serious risk to the horse’s survival and requires immediate surgery to attempt to clean the exposed bowel and return it to the abdomen. Fortunately this is extremely rare in the Thoroughbred.
However, the most common complication is infection at the site of the castration. This procedure leaves an open wound and obviously the horse can lie down in bedding full of urine and feces on the same day it has been castrated, therefore potentially contaminating the open surgical site. Unfortunately many racehorses’ ability to be turned out in a paddock is often controlled by the training environment they reside in. Infection post-castration, and the added expense and lost training days associated with it, is a bugbear for trainers and vets, and this study reviews a common problem encountered worldwide.
Hong Kong Study
The Hong Kong training complex provides full-time stabling and training facilities to approximately 1250 horses spread out among 24 licensed trainers. The Department of Veterinary Clinical Services (DVCS) at the HKJC is the sole provider of veterinary care for this population. All clinical records of horses in training at the HKJC are collated within the Veterinary Medical Information System (VMIS). For a horse to be eligible for inclusion in the study, two testicles had to have been removed via an open standing castration. Veterinary records of all the horses that had been castrated were examined and any cases that did not meet the criteria were excluded.
Data on complications that occurred in the 30 days following castration was extracted from the clinical notes in the VMIS. The data was reviewed and the severity of complication was categorized into one of the five groups below:
Between July 2007 and July 2012, 280 racehorses in training were castrated. A total of 30 horses were omitted from the study, as they did not meet the inclusion criteria: 24 horses were castrated using general anesthetic, of which six were cryptorchid surgeries. Horses included in the study were in the care of 24 different trainers, with thirteen different veterinarians performing the castrations.
Twenty-four hours after castration, this horse has mild scrotal swelling, which would be classed as Group C1 in the Hong Kong study.