These scales were used in a recent Equine Veterinary Journal article looking at optimal methods to provide anaesthesia for castration. But, the focus on a strained facial expression, ears held back and lack of interaction with people can easily be misinterpreted as poor temperament. It is well worth trainers taking time to make sure their staff are educated on how to recognise signs of pain, as these sorts of clinical signs might indicate important conditions such as gastric ulcers, pneumonia or even musculoskeletal conditions such as fractured ribs. Yard staff should be encouraged to give horses the benefit of the doubt and report any apparent poor temperament so that veterinary investigations can be undertaken to get to the bottom of the problem. Similarly, these signs can be used to monitor horses after potentially painful procedures such as following surgery or castration.
What do we know about analgesic use in equine practice?
There is an increasingly large number of painkillers, also known as analgesics, which are either licensed for use in the horse or supported by research evidence. But it is likely that most equine vets use a relatively small range. British Equine Veterinary Association (BEVA) has recently tasked a team of its members to look at the evidence with underpin best practice for selections of analgesics in common clinical scenarios. This group is chaired by Professor Mark Bowen of the University of Nottingham and has been working for two years now and has collected evidence from the veterinary literature; and in parallel the group has consulted BEVA members to develop robust recommendations. The BEVA Clinical Practice Guidelines report on analgesia will be published soon and looks at the most effective analgesia in horses undergoing routine castration, horses with acute colic, orthopaedic pain and in horses with chronic pain that does not respond to standard non-steroidal anti-inflammatory drugs (NSAIDs) such as phenylbutazone (aka “Bute”). In making their recommendations around use of analgesics in horses, the BEVA team considered both the effectiveness of each analgesic drug, its safety and potential for side-effects.
What are the desirable characteristics of analgesic drugs?
The ideal analgesic has predictable effect and duration, minimal side effects and is easy to prescribe, purchase and administer, lacking any impact on the horse’s future status for human consumption. Of course, the ideal analgesic does not exist. To a large extent, the most appropriate analgesic will be dictated by the specific clinical indication.
Analgesia in colic
With colic, predictable level of analgesia and duration of action are key characteristics. The BEVA team found moderate evidence that flunixin provides superior analgesia to meloxicam and phenylbutazone in horses with colic. However, effective analgesia is desirable but very potent drugs are usually avoided for fear of masking declining clinical status in a horse which would be best served by surgical exploration rather than controlled with extremely potent analgesics. Potential damage to the gastrointestinal tract and effects on gastrointestinal motility are critical and the impact of concurrent shock and volume depletion must be considered. Similar considerations come into play with peri-operative pain but here, the level of analgesia required may be modified by the exact surgical indication and specific procedure and with some procedures, it will be appropriate to provide very potent analgesia, for example with surgical repair of fractures or other painful orthopaedic surgeries. In these cases, multimodal analgesia may well be indicated.
Analgesia following castration
The BEVA team found robust evidence to support a recommendation that pre-operative NSAIDs should be administered prior to surgery. They also recommended that analgesia should be given for at least three days after surgery and that local anaesthetic should be infused into the testicle even when a general anaesthetic is administered. Finally, they counselled that pre-operative use of butorphanol (a commonly used component of sedative protocols) alone should not be considered adequate analgesia for horses undergoing castration.
Selection of NSAIDs for musculoskeletal pain
There is moderate evidence to indicate that phenylbutazone provides superior analgesia for hoof pain / laminitis, compared to firocoxib and meloxicam but strong evidence to show that Suxibuzone can be used as a direct replacement for phenylbutazone in chronic orthopaedic pain. The evidence supporting the use of other NSAIDs is less definitive. Meloxicam and firocoxib may be equivalent to phenylbutazone for pain associated with inflammation of the joint lining and, although studies are not conclusive, the group came to the conclusion that ketoprofen is not as effective for addressing musculoskeletal pain.
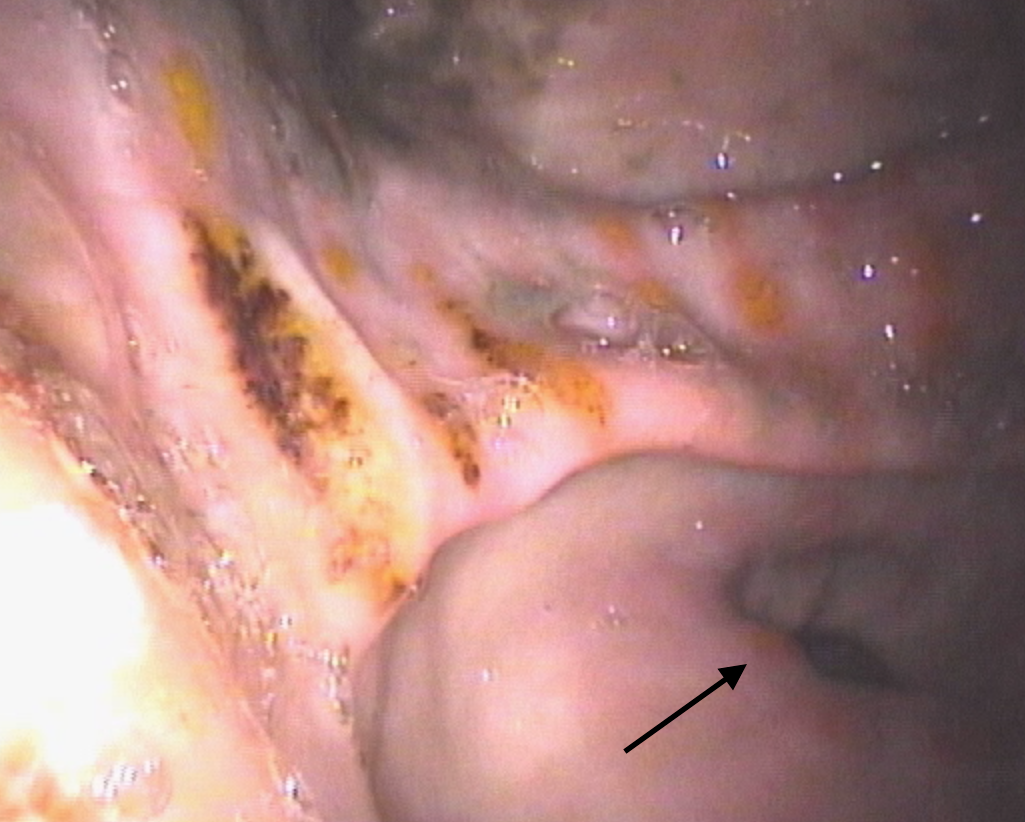
One of the key safety recommendations relating to the use of phenylbutazone was that it is the NSAID that is most likely to induce gastrointestinal adverse events (right dorsal colitis or gastric glandular ulceration). However, although other NSAIDs have less adverse intestinal effects but can all be considered as potentially ulcerogenic. Horses on long-term analgesic therapy should be monitored carefully and further investigations undertaken if they show weight loss, poor appetite or develop the more general signs of pain described above, as this might indicate that the NSAID is having adverse effects on the intestine.
The BEVA team also concluded that giving NSAIDs at doses above those generally recommended in veterinary texts and stacking (i.e., combining maximal doses of different NSAIDs) should be avoided. These practices simply increase risk with no analgesic benefit.
Alternative analgesics
Unfortunately, there are not many practical alternatives to NSAIDs. There is research ongoing looking at topical NSAIDs and alternative drugs such as paracetamol, tramadol and fentanyl. These drugs are unlikely to be in common use in horses in training but do have a place in management of horses with more severe clinical problems.
Similarly, morphine and methadone are used commonly in equine hospitals, but these Schedule 2 controlled drugs are generally not used widely in practice. Buprenorphine has been extensively researched recently and evidence is accumulating supporting its use particularly in the peri-operative patient.
Final warnings
The BEVA group’s report contained a clear warning that highly potent analgesia should only be utilised under the direct control of a veterinary surgeon who has fully evaluated a horse and having developed a therapeutic, analgesic plan that includes ongoing monitoring. It is also important to bear in mind that the best way to alleviate pain associated with a specific clinical condition is to cure the underlying cause. Painkillers should always be used with respect and not be seen as a way to patch up a horse that has an undiagnosed musculoskeletal problem or internal condition.
BUY THIS ISSUE IN PRINT OR DOWNLOAD